scott@vtx-cpd.com
Forum Replies Created
-
AuthorPosts
-
Replying to Liz Bode 01/09/2024 - 20:38
Hey Liz!
Fancy seeing you here!
Scott 🙂
Replying to Anna H. 01/09/2024 - 20:39
Hi Anna,
Welcome to the course! It sounds like you have a wealth of experience, and it’s great to hear you’re embracing the challenges of GP practice. I’m sure the course will be a great way to refresh your knowledge and boost your confidence after returning from maternity leave. Looking forward to learning alongside you and sharing experiences!
Let me know if you have any questions.
Scott 🙂
Replying to Karin V. 04/09/2024 - 13:01
Hi Karin,
I’m also looking forward to hearing Liz’s perspective on this topic, but I thought I’d share some of my own insights. From my experience, tracheal stenting can be a life-saving procedure for patients with very severe tracheal collapse. However, I often see referrals for patients with suspected tracheal collapse, even in the early stages, where stenting is being considered as though it’s a universally life-improving procedure that can be done at any time without complications. That’s simply not the case, and I think this paper highlights that well.
For me, it’s crucial to optimize medical management first, using combinations of antibiotics, steroids, and antitussive medications before even considering tracheal stenting. In my experience, many patients can be managed well for quite some time on medical therapy alone, even those with more advanced disease.
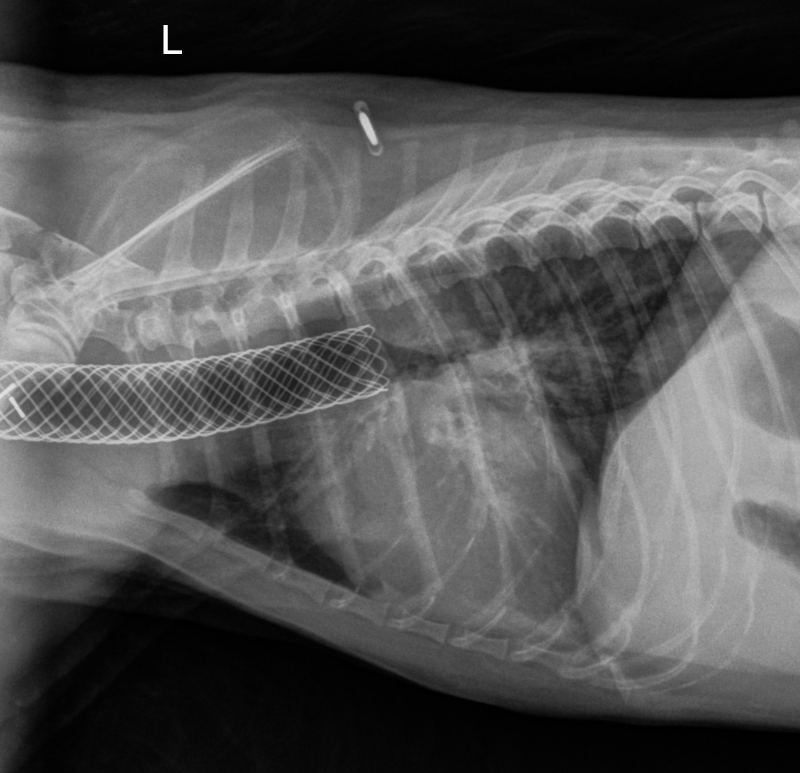
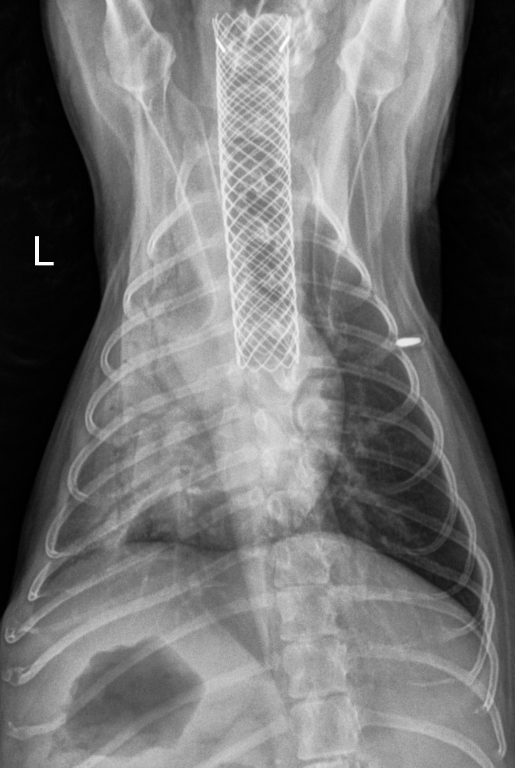
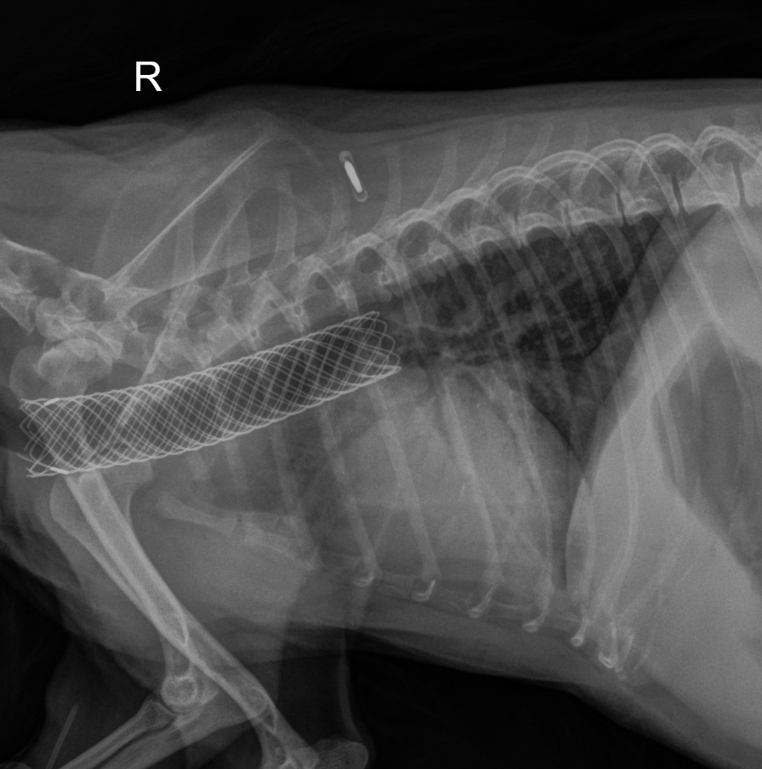
I actually have a patient this week (I’ve shared the radiographs below) who had a tracheal stent placed about two years ago but continues to experience recurrent bouts of bronchial pneumonia. This patient still coughs even with the stent in place, which is an important consideration when discussing long-term outcomes.
Looking forward to hearing your thoughts!
Best,
Scott
Replying to Karin V. 02/09/2024 - 19:19
Hi Karin, welcome to the course! It’s great to have you with us, and I’m sure your background in both clinical and industry roles will bring some valuable insights. Looking forward to learning and sharing experiences together. If you need anything, don’t hesitate to reach out!
Scott 🙂
Replying to Ingrid T. 06/09/2024 - 20:39
Thank you so much Ingrid!
We appreciate you!
Scott 🙂
Hi Rosanna,
Thank you so much for your question and for your continued support of VTX. We truly appreciate it!
There won’t be a live Q&A session associated with the course this year. In the past, we offered live Q&A sessions for many of our courses, but based on delegate feedback and challenges with attendance, we decided to remove it from some courses, including the dentistry course. Instead, we encourage using the discussion forum for any questions you may have, which has worked well for many delegates.
That said, we’ve tried to introduce other live elements to make up for the lack of Q&A sessions. For example, we’ve added live events such as the Cytology Rounds, Radiography Rounds, and Round Table Discussions, which provide interactive experiences and opportunities for engagement.
We’d love to hear your thoughts! If you feel that a live Q&A would be beneficial, we can certainly consider that for future courses. Your feedback is always valued, and we hope you’re enjoying the course overall.
Best regards,
Scott
Replying to Jenny G. 06/09/2024 - 15:04
Welcome Jenny!
Amazing to have you here!
Scott 🙂
Replying to Rosanna Vaughan 06/09/2024 - 11:10
Hey Rosanna, thanks so much again for your question! Ingrid has kindly added the links below—I hope they’re helpful. Please let us know if you need any more information.
You’ve raised an interesting point about dental or local nerve blocks, and this might be an area where we could provide more focused teaching. We’re definitely considering developing a webinar specifically on this topic, and it’s something we could also potentially include in future practical sessions. Let me know your thoughts on that!
Scott 🙂
Replying to Hannah Willetts 05/09/2024 - 09:09
Hi Hannah,
No problem at all! I’m glad the information was helpful. Feel free to reach out anytime if you have any more questions or need further clarification.
Thanks again,
Scott 🙂
Replying to MARK C. 03/09/2024 - 03:21
Hello Mark!
So wonderful to have you join us. We are very excited to work with you!
Radiography is an ongoing challenge for many of us… I am speaking for myself here!
It is wonderful to have your expertise!
Scott 🙂
Replying to Felipe M. 03/09/2024 - 09:09
Felipe!
So wonderful to have you join us… as always!
We really appreciate your brilliance and support!
Thank you.
Scott 🙂
Replying to Ingrid T. 03/09/2024 - 09:19
Thank you!
I will ask the delegate for these and get back to you.
I hope you are having a great week.
Scott 🙂
Replying to Dan T. 03/09/2024 - 17:06
Welcome Dan!
Thank you again for working with us on this brilliant course!
Hope you are having a great week.
Scott 🙂
Replying to Dan T. 03/09/2024 - 17:12
I agree!
Jenny has a wonderful way of reassuring us too! I have also done some personal coaching with Jenny and she has a wonderful way of making things make sense!
Scott 🙂
Replying to Dan T. 03/09/2024 - 17:24
Hi Dan,
Thanks for your thoughtful response. Core values can be a powerful tool for both individuals and organizations, even though they can sometimes feel hard to define or align perfectly within a team. I love how you highlighted the challenge of balancing personal values with organizational ones. When those values are communicated clearly, even if not perfectly aligned, they can still provide that crucial reference point for decision-making and a sense of belonging.
I’m also curious to hear how others have approached identifying and integrating their own values into their work.
Best,
Scott -
AuthorPosts