scott@vtx-cpd.com
Forum Replies Created
-
AuthorPosts
-
Replying to Georgia 21/03/2025 - 16:00
Thanks for the reply!
I did see that JFMS had just published this article this week:
https://pmc.ncbi.nlm.nih.gov/articles/PMC11874005/pdf/10.1177_1098612X251320877.pdf
Scott 🙂
Replying to Laura S. 21/03/2025 - 18:03
Hi Laura,
Ah, thank you for sharing this. I’m genuinely disappointed (and a little deflated) to read the JFMS study. It very much doesn’t support the use of intranasal maropitant, despite all the anecdotal promise and theoretical basis we’d been leaning on. I had completely missed this paper, so I really appreciate you and your colleague bringing it to the table.
So now we’re left in a tricky spot. The evidence says “no benefit,” but part of me still wonders if there’s a place for it in the most refractory cases, where we’re trying to do something to help these poor cats breathe. Of course, any use now really has to be framed as off-label and not evidence-supported, and I think this study will rightly temper some of the optimism that’s been floating around.
Thanks again for sharing. I’ll share it in other forums too.
Scott 🙂
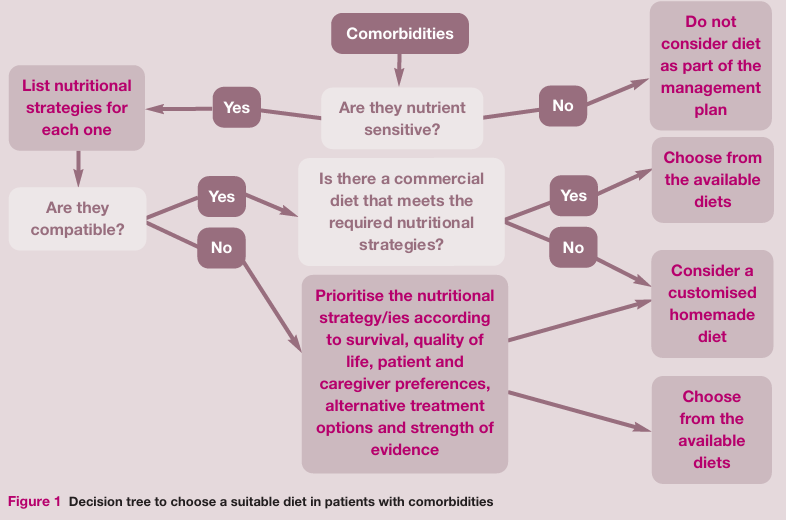
This is a great question!
I must admit I often panic. I find myself prioritising the most life threatening issue… but I fear that this may be the wrong approach!
I think the one that probably comes up most for me is kidney. For example, I have a patient at the moment with chronic kidney disease but also some really severe skin issues/allergies. The other one that comes up quite a bit is when patients are on a hydrolysed protein for GI issues and then develop another problem.
I often will call the food companies. I find Hills and RC very helpful! I feel less people go for the home cooked/formulated option but I always offer it.
Scott 🙂
Replying to Georgia 17/03/2025 - 09:45
Love the fibre chat!
I do tend to recommend a lot of people to add psyllium or pumpkin to the diet. What are your thoughts on pumpkin? Also, with the psyllium, what amounts do you normally recommend?
There are a few veterinary fibre blend supplements out there too, I think Protexin might make one. What do you think of those?
Scott 🙂
Replying to Raquel M. 20/03/2025 - 12:34
I think that is a great questions generally!
I always try and advocate charging for this sort of time. We have a cost for a technician appointment. It is around $50 Canadian Dollars. This would normally be what we charge for this sort of thing.
If this is for a patient that has been hospitalised or been in for a procedure we would often do it as part of the discharge process without additional charge.
Scott 🙂
Hi Kerida,
Hope you’re doing well! How’s life in practice treating you?
With rectal diazepam becoming unavailable, a lot of us are turning to intranasal midazolam as an alternative for at-home seizure management in epileptic dogs. There’s good evidence supporting its use, with studies showing it achieves faster seizure cessation than rectal diazepam and tends to have fewer adverse effects. A study in the Journal of Veterinary Internal Medicine found that intranasal midazolam was as effective as rectal diazepam in managing canine status epilepticus, which you can read more about here: https://pubmed.ncbi.nlm.nih.gov/28543780/.
For administration, the standard dose is 0.2 mg/kg intranasally using a mucosal atomization device, which ensures good absorption. This is backed by research discussing the various administration routes of benzodiazepines in dogs: https://pubmed.ncbi.nlm.nih.gov/33663513/.
Rectal diazepam tablets are not recommended for rectal administration due to inconsistent absorption and efficacy. A systematic review with meta-analysis highlights the effectiveness of non-intravenous midazolam compared to rectal diazepam: https://pubmed.ncbi.nlm.nih.gov/25817929/.
The big advantages of intranasal midazolam are its rapid onset and ease of use. Since it’s absorbed quickly via the nasal mucosa, it tends to work faster than rectal diazepam, which is crucial in an emergency. The Journal of Veterinary Internal Medicine study backs this up: https://pubmed.ncbi.nlm.nih.gov/28543780/. It’s also a lot easier for owners to administer, especially compared to trying to give something rectally mid-seizure. This is further discussed in the review on benzodiazepine administration: https://pubmed.ncbi.nlm.nih.gov/33663513/.
If you’re switching owners to intranasal midazolam, it’s worth taking some time to train them on how to use the atomization device properly. They also need to know what to look out for in terms of side effects, like sedation or nasal irritation, and when to seek further veterinary care if seizures persist.
Overall, intranasal midazolam seems to be a reliable and effective alternative to rectal diazepam for at-home seizure management. It’s great to have a practical option that works well in these cases.
Hope that helps. Let me know how you’re getting on.
Scott 🙂
Replying to Gemma B. 19/03/2025 - 15:38
Hey Gemma!
This is really interesting. I wonder what is is about the j/D that makes it more palatable?
I suppose my question would be… why do they not just add that to all the kidney diets!?
Scott 🙂
Replying to Raquel M. 19/03/2025 - 15:50
Hey Raquel.
You can access the recording here:
https://vtx-cpd.com/webinars/?filter=Caesarean
Scott 🙂
Replying to Raquel M. 19/03/2025 - 21:17
Thanks Raquel.
I think the time element is one of the biggest issues.
This is definitely not the sort of thing that can we rushed.
We will often book a separate appointment just to go through training and using the inhaler.
Scott 🙂
Replying to Raquel M. 18/03/2025 - 15:13
That’s a great point, Raquel. Hydracare definitely seems to be hit or miss with individual cats, but for the ones that take it, it’s an easy way to increase hydration without needing to resort to SQ fluids. I agree that simplifying the dosing to one pouch SID regardless of size is a practical approach—getting owners to stick with it consistently is often more valuable than perfect adherence to the recommended amount.
I haven’t seen much recent research on its efficacy either, but anecdotally, I’ve seen it help in some cases. Interesting that some vets have used it in dogs as well—I imagine it could be useful for chronic kidney disease patients or those needing extra hydration support without IV or SQ fluids.
Clients are already prone to selective hearing, so if different team members say slightly different things, it makes it even harder for them to understand the importance of environmental changes. I think your approach of giving them the resources and accepting what’s out of your control is the best way to handle it—it’s all we can do sometimes!
Scott 🙂
Replying to Laura S. 18/03/2025 - 14:52
That’s such a great point, Laura, and definitely something I run into as well. Clients often struggle to see stress as a factor, especially when they perceive their cat’s life as comfortable or don’t notice overt stress behaviours. It can be tough to explain that what we see as a calm environment isn’t necessarily what they experience.
I think handing out the ICC client guide is a great idea, but I agree—getting them to actually read it is another challenge. Sometimes, I find that framing it in terms of predictability and control rather than outright calling it “stress” helps. Instead of saying, “your cat is stressed,” I try to ask questions like:
Does your cat ever sit and stare at you before eating? That’s a sign they might be food-motivated but also anxious about when their next meal is coming.
Does your cat follow you to the bathroom? That’s often a sign they’re seeking security and reassurance.
Ever seen your cat sprint across the house out of nowhere? That could be a stress outlet, not just zoomies!
I love Sarah Caney’s stance, letting cats go outside or bringing the mice in is a hilarious but effective way to get the point across!
If you haven’t already, you should check out the latest podcast about these very guidelines with Sam: https://podcasts.apple.com/us/podcast/episode-70-just-a-thought-should-i-use-prazosin-in/id1514839581?i=1000699372600.
Scott 🙂
Replying to Cristina M. 14/03/2025 - 15:45
Hi Cristina,
That’s really interesting to hear about the approach in Italy. It makes sense that prevention efforts are keeping cases relatively low, which probably reduces the need for routine testing before surgery. I can see how it’s a difficult balance between identifying at-risk patients and adding unnecessary screening.
I’ve definitely seen more issues with lungworm-related coagulopathies in the UK than heartworm, and I agree that testing before abdominal procedures seems like a good precaution in those cases. I wonder if there will ever be a clearer consensus on pre-surgical screening for both heartworm and lungworm, or if it will always come down to clinical judgment and local risk.
Scott
Replying to Liz Bode 13/03/2025 - 21:13
HAHAHAHA!
Me too!
Scott 🙂
Replying to Laura S. 11/03/2025 - 20:03
Hi Laura,
Great to hear your thoughts. I’m the same, I’ve never really looked for hypernatremia after AC either, and it’s not something that’s been flagged as a major concern when following VPIS advice. It’s interesting that your formulation contains glycerine rather than sorbitol, I wonder if that has any impact on sodium shifts.
I tend to stick to one or two doses unless enterohepatic recirculation is a factor, and then I’d usually go for every six to eight hours for three doses rather than continuing indefinitely. I guess it’s always a balance between risk and practicality.
This study is really interesting because it suggests that single-dose AC may be just as effective as multiple-dose AC in reducing overall plasma drug exposure in carprofen overdose. All AC protocols, including single-dose and multiple-dose AC, significantly reduced overall carprofen exposure compared to controls, and while multiple-dose AC shortened the half-life, it did not significantly outperform single-dose AC in lowering total drug exposure. From a practical standpoint, this could make AC administration more manageable, particularly in outpatient cases where multiple doses may not be feasible.
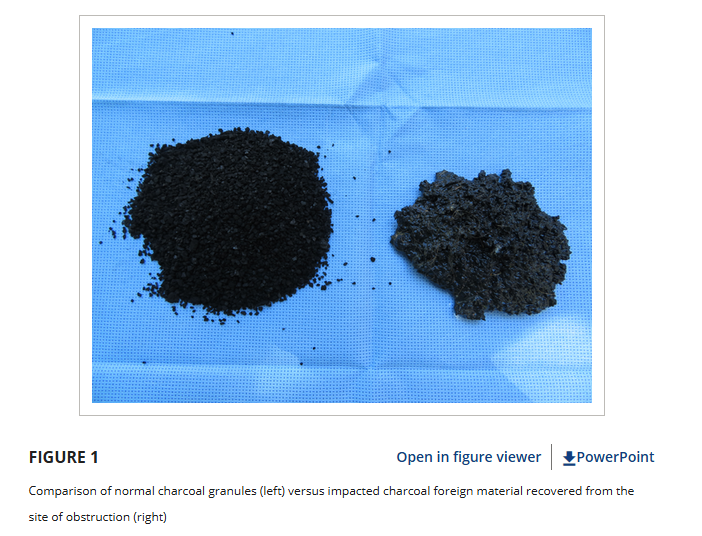
While looking into this, I also came across a case report of gastrointestinal obstruction secondary to activated charcoal granule impaction. A two-year-old Airedale Terrier received multiple doses of AC granules for carprofen toxicosis and ultimately required surgical removal of impacted charcoal material from the ileum. Not something we see every day, but definitely a reminder that more is not always better when it comes to AC.
And yes, it is always a light-coloured dog, isn’t it? Never the black Labs.
Scott
Full papers:
Carprofen overdose and AC effectiveness: https://onlinelibrary.wiley.com/doi/10.1111/vec.12305
Case report of AC impaction: https://onlinelibrary.wiley.com/doi/10.1111/vec.12980Thank you again for another brilliant video on a really interesting topic!
Scott 🙂
-
AuthorPosts