Liz Bode
Forum Replies Created
-
AuthorPosts
-
Hi Sarah
Great question and really that’s incredibly difficult. The only way is to treat the hyperthyroidism etc and see if the HCM regresses. If it’s secondary then the heart will normalise over time. Anecdotally, I think most cats have a mixture of both so never fully reverse remodel.
Liz
Replying to Liz Bode 17/09/2023 - 15:49
As this course is drawing to an end I thought I would close this case 🙂
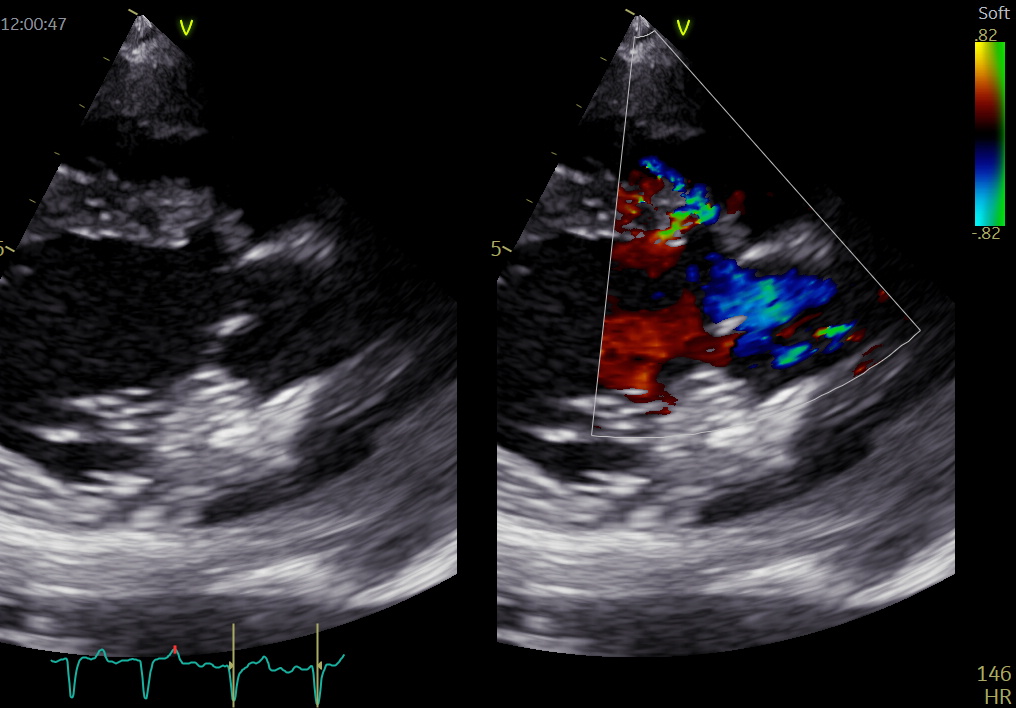
the image shows a large (1cm) VSD in the perimembranous region. It is classified as an inlet VSD as it occurs where blood moves from the RA to the RV (inlet septum) rather than the outlet septum where blood is moving from the RV to PA. The Doppler shows a L-R shunt and the shunt was significant enough to be causing volume overload of the left side. This, in turn, has resulted in the AF.
We don’t see many cases such as this and I am currently waiting to see if the RVC could fix the defect under bypass..
Replying to Sarah Keir 24/09/2023 - 12:34
Hi Sarah,
Unfortunately, rivaroxaban is also bitter to taste! So some cats may not tolerate either.
I generally will give both to cats that have a thrombus or very poor LA function that have already suffered an ATE episode. Otherwise I tend to just use clopidogrel. There is no evidence for the use of clopidogrel prior to ATE so we don’t really know how much, if any, difference it makes but it makes us feel like we are doing something at least.
Liz
Hi everyone,
I’d also like to welcome you all to this brand new course, it will be fantastic! I’m Liz, one of the other Director’s of vtx and a cardiologist. I’m available to answer any questions that you might have with regards cardiology!
Enjoy the course, and as always, we welcome feedback about other content you might want to see on here.
Liz
Replying to Sarah Keir 17/09/2023 - 19:02
Hi Sarah
Yes, it will be years (if at all) before this drug hits the veterinary market. So many more stages to pass through and the data wasn’t overwhelming for me. Still interesting though! Let’s hope larger studies show similar (or better) findings.
Are you doing the Improve course with Cambridge? They’re a lovely group 🙂
Liz
Replying to scott@vtx-cpd.com 17/09/2023 - 19:15
Hi Scott
It’s available in the human medicine world but as far as I’m aware we don’t use it in veterinary yet. As I said, it’s a pilot study so much more data is needed before it becomes mainstream 😉
Liz
I agree! The systolic function looks OK and so excludes DCM. A congenital condition is very likely here. SAS usually causes concentric hypertrophy, which isn’t present, but at end-stage SAS you get what we call ‘myocardial mismatch’ or ‘afterload mismatch’ where the walls actually become thinner due to replacement fibrosis. So, you could see normal/ thin walls with even severe SAS. In my mind though this left side looks volume loaded, so we are thinking about a disease process that is congenital and causes volume loading of the left side…it will become clear (hopefully) with these videos…what do you think now?
https://drive.google.com/file/d/1UJWZeF3nPodqAGy01Bh4YdXkG2NyaZi7/view?usp=drive_link
https://drive.google.com/file/d/1G1Kvx4VC2ehmTTHMkcXNVe_vd1sYk5K9/view?usp=drive_linkIn terms of the interatrial septum, you often get echo dropout around the middle of the septum. If you think there is an ASD you need to identify it on 2 views to make sure it isn’t an artefact 🙂
Hi Natalie,
Some great questions, treating cats is confusing with little or no evidence for very much!! I will answer each question in turn:
My understanding from the lectures is that all cats in congestive heart failure get frusemide at lowest effective dose.
Yes, that’s correct. We will cover this later in the CHF section. However, as a rule of thumb I use 2mg/kg PO BID (TID if they were difficult to control) and then once I am happy the cat is stable I will try and reduce the dose to lowest effective, although not really below 1mg/kg BID.Those with evidence of smoke / spontaneous contrast on echo get clopidogrel to reduce risk of thrombus.
Yes, clopidogrel is the one we choose as we have evidence for its use from the FATCAT study (2015) in recurrent ATE events. So, I prescribe it to cats with moderate dilation of the LA, smoke, or poor LA systolic function.Do you ever use aspirin in these cases?
Not really, no. the therapeutic index isn’t very high (its not COX selective) and I would prefer to use clopidogrel with rivaroxaban (a factor Xa inhibitor) or one or the other. I might use aspirin if the cat is very difficult to tablet though, as better than nothing probably (although we don’t know this either!).I know a lot of clinicians use every third day (think it’s a quarter tablet?). Can this be given in combination with clopidogrel?
Yes, you can use it in combination with clopidogrel as they work in different ways.You said there’s no good evidence that ACE inhibitors such as benazepril improve survival so we should not give these unless hypertensive?
I will use an ACE inhibitor if the cat isn’t doing very well, but the King paper suggests that including an ACE inhibitor has no benefit either before CHF develops or during CHF. I will use spironolactone though as there is a (poor) study that suggests some benefit, but what I really use it for is boosting the potassium levels.And pimobendan is contraindicated unless it is DCM which is much rarer.
It’s not contraindicated per se, it is just that there is no evidence that it works. This makes sense as pimobendan increases contractility but HCM is a diastolic disease. a recent paper showed no benefit in using it in cats with HCM to 180 days, so it is going out of fashion. I would definitely use it in a cat with DCM though, or possibly end-stage HCM where you see poor systolic function secondary to myocardial ischaemia.Then where I’m a little confused is – do you use beta blockers such as atenolol only in obstructive hypertrophic cases where there is systolic anterior motion, and then diltiazem in HCM cases without obstruction to improve diastolic filling? Or am I mixed up?
Yes, atenolol only in severe HOCM. Again, no benefit here but physiologically it makes sense to use a beta blocker. You need to demonstrate the severity of the obstruction via Doppler though before prescribing it. We don’t use diltiazem in cats, unless they have an arrhythmia. It used to be prescribed for HCM as the thought was that slowing the HR down would improve myocardial perfusion, but it is TID dosing and there is no evidence that it works.Hope that clears things up for you 🙂
Liz
Hi Natalie,
So there is one loop only (I’m on holiday this week but will add more next week once I’ve got my laptop). In this loop you can see left atrial and ventricular dilation with normal systolic function. There is also AF on the ECG. The MV is slightly thickened but isn’t the concern in this dog. Any other thoughts as to processes that could cause these findings in a dog with a loud murmur?
Liz
Replying to Natalie Niven 07/09/2023 - 17:01
Hi Natalie,
I’ve not seen one performed in dogs, only people, but the procedure is the same for both. They use cardioplegia and then place catheters within various vessels and circulate the blood through the bypass machine. The heart is approached via the left atrium and as this is a low pressure chamber with thin walls you can suture it up with little risk, but yes that will always be a risk. The main risk though is thrombosis following recovery and these dogs are given clopidogrel to prevent it. They then repair the valve by placing new chordae to tether the valve again.
Yes, with decompression that is what you do. 30% have R CHF afterwards, but this is easier to manage than L. 30% close up. We don’t have any evidence as to whether they do better than meds alone but this technique is used in people too.
Scott – that’s a great episode of Grey’s!
Liz
Hi everyone
Great to have you all join us on this course. I’m Liz, one of the directors of vtx but also a specialist in cardiologist working in private practice in the NW of England. Please feel free to ask me anything cardio related.
Liz 🙂
Replying to scott@vtx-cpd.com 03/09/2023 - 20:11
Yes, they were the pioneers of the approach and for realising replacement was not as good as repair in dogs in terms of survival post surgery.
Replying to scott@vtx-cpd.com 30/08/2023 - 10:52
Hi Scott,
We haven’t had a suitable candidate yet, but we would certainly be able to try left atrial decompression in a suitable stage C/D candidate.
Repair would be my overall preference, they are having some good outcomes with reverse remodelling and many come off medications. TEER is similar in USA but is in the very early stages in UK.
I haven’t sent any dogs yet, cost is almost prohibitive for many owners in UK where they are not used to paying such high bills for health care vs the USA.
Liz
Replying to scott@vtx-cpd.com 29/08/2023 - 14:20
Hi Scott
That’s hard to answer. If o hear a right sided systolic murmur in a cat I will try and press less hard to see if the murmur goes away. The same when I’m performing echo, if I see turbulence in the RV outflow tract I’ll try and press less hard to see if the turbulence resolves.
Liz
Replying to scott@vtx-cpd.com 29/08/2023 - 16:56
Hi Scott
Unfortunately for the owner it was detected 3 weeks after he rescued him at a routine vaccination. The dog is asymptomatic at present 🙂
Liz
-
AuthorPosts