Liz Bode
Forum Replies Created
-
AuthorPosts
-
Replying to Emma Riley 02/06/2026 - 11:38
Hi Emma,
I will reach out to Sid and get back to you once he has responded.
Liz
Sorry this took so long to reply too, I was waiting for info from Oscar as it was beyond my expertise 🙂
Hi Julia,
Great question – it’s a really interesting point and one that’s a bit controversial taking into account how we’re usually taught to be cautious with alpha-2s in cardiac patients.
What I meant is that the effects of dexmedetomidine (and medetomidine as well) are very dose-dependent. At “normal” doses or when given as a bolus, you get the classic picture – peripheral vasoconstriction, reflex bradycardia, and a marked reduction in cardiac output. That is obviously not ideal in many cardiac cases.
However, if you use very low doses as a CRI, you could avoid that plasma peak increase and mainly get the central effects (sympatholysis) without much peripheral vasoconstriction. In practice, that means less catecholamine release, less tachycardia (and bradycardia), reduced myocardial oxygen demand, and generally smoother haemodynamics. That’s where the idea of “cardioprotection” comes from.
In terms of when to use it, I usually think about relatively stable cardiac patients (for example compensated MMVD) where tachycardia or stress responses could be contradictory. It’s not something I would use for in unstable patients. I’d usually start the CRI after induction, once things are stable, and use it as part of maintenance to help with surgical stimulation and reduce inhalant requirements.
For dosing, a typical dexmedetomidine CRI would be around 0.25–1 µg/kg/hour, starting at the lower end and titrating to effect. The aim is trying to remove its sympathetic tone if that makes sense. If dexmedetomidine is not available, medetomidine can be used doubling the dose.
So overall, it’s less about using alpha-2s as “sedatives” and more about using them as a very fine-tuned way of controlling sympathetic tone.
Hope that helps a bit – it’s definitely one of those areas where small dose titration make a big difference!
Thank you
Oscar
Replying to Julia Biernat 11/04/2026 - 09:14
Hi Julia,
No problem!
1. Can we tell from these that the Vtach is right sided? The complexes are positive in lead II which would suggest that these complexes come from the right ventricle.
2: I calculated the HR at 180 is that correct? counted 10 large squares as 1s. I don’t tend to count the squares on an ECG like this, my eyes always make me get different answers from a screen (I am old fashioned an need a printed copy). If you look along the very top of the ECG you will see some markers and numbers after them. These markers correspond to the QRS complexes and are in milliseconds. You can work out an instantaneous rate by dividing 60,000 by the number e.g. 60,000/ 230 = 260bpm.
3: Can we tell from these that it’s Mobitz type II and that’s more advanced disfunction than type I or does it not really matter? This looks like Mobitz Type I – the PQ interval appears to prolong slightly before the blocked P wave and then the PQ after the blocked P wave is shorter again, characteristic of Mobitz type I which tends to be more physiological. Type II tends to be more pathological (although not always pacemaker territory).Hope that helps.
Liz
Replying to scott@vtx-cpd.com 30/03/2026 - 00:31
Our anaesthetists would use dexmedetomidine (or other alpha-2) in cats with HCM, the main reason being is that HCM is a disease of diastolic function and systolic function is often preserved (unless end-stage), so the alpha-2s will have limited adverse effects on cats. They usually use a low dose (I am sure Oscar discussed this in his webinar), together with an opioid. Cats also less commonly have mitral regurgitation, which would be another contra-indication to using this class of drug (they increase afterload and so can worsen regurgitant fraction through the mitral valve).
Thanks for sharing! Yes, this is what we already know, that systolic function cannot be interpreted. Its use in cats is less worriesome as they have diastolic disease (although they can get issues with systolic function too).
LizHi Scott,
This is interesting, thanks for posting.
Monitors like this have been around in people for years, they are often used as part of pacemaker technology and are used for a similar reason; to alert clinicians when early congestion might be present. Their use in dogs and cats has been limited by the fact that they were designed for human chests, measuring changes in impedance with respiration, but had never been validated in dogs before. They were known to be inaccurate in dogs because of panting and movement issues. It is interesting that this collar doesn’t appear to work via impedance (not that I could see from their website at least), and good that it records resting/ sleeping breathing rates. It is a clever subscription service for the worried owner I guess! My feeling is that an owner that invests in such technology would be the more motivated owner regardless, and so might not be a great use of money in terms of they would then be more likely to monitor RRR anyway!
Will be interesting to see take up!
Liz
Hi Julia,
This sounds like a tricky case indeed.
It could be an LA rupture, if the effusion was big enough it might have been causing some limitation to LA size/ the left side might be under-filled due to blood loss. However, normally dogs with LA rupture have significant LA dilation, which is what leads to wall thinning. Often, but not always, you will see a thrombus within the pericardial space as one clue. I think B-lines around the pericardial sac can be misleading. There is a paper that suggests they are conducive to CHF, but in my experience you frequently see B-lines around the heart in normal dogs.
I guess in this case, where I wasn’t sure of the cause but there was significant effusion with tamponade I would attempt to drain it, monitoring carefully for the appearance of a thrombus, so doing it ultrasound guided would be preferable here.
Poor dog, sounds like she was quite poorly!
Liz
Replying to Julia Biernat 20/02/2026 - 12:31
No problem at all!
Yes, it is always a good one to warn owners about. I always say that some ‘idiopathic’ cases will be mesothelioma in the end and we do not have a good way of identifying which cases have it and which don’t!
Replying to Silvana S. 21/02/2026 - 19:46
Hi Silvana,
Welcome, we are really pleased that you have joined us and are starting to use the platform etc. Those are some great suggestions, and we can certainly look to incorporate more of those topics over the next year.
Let us know if you have any further suggestions/ queries or if we can help at all.
Liz
Replying to Ornella R. 15/02/2026 - 21:59
Hi Ornella,
Glad you have found it useful.
Each lecture should have it’s own downloadable pdf? If you can’t access them please let us know.
Liz
Replying to Annet Krabbenborg 16/02/2026 - 12:57
Hi Annet,
Good question! Yes, they have been shown to have larger LV than other dogs. We would still use the EPIC criteria though to determine when to start pimobendan, but we might reassure some owners that the LV isn’t that big in reality!! It is confusing. The study wasn’t one looking at CKCS in particular, but Mark Rishniw demonstrated that as a breed CKCS have LV that are often larger then the 1.7 EPIC cut off!
This was the paper:
https://www.sciencedirect.com/science/article/abs/pii/S1760273422000595?via%3Dihub
Liz 🙂
Replying to Ornella R. 15/02/2026 - 21:51
Hi Ornella,
When measuring turbulent jet velocity: we identify the jet with colour doppler and in order to get an accurate velocity, we place the CW gate in the neck of the jet (vena contracta), is this correct?
Yes, that is correct, or just on the atrial side of the valve within the colour variance if there is TR or MR.
When measuring PA and AO velocities with CW or PW: do we place the cursor gate across the valve, just below or just above?
This depends on where you see the colour variance start. For the most part the turbulent flow will be within the major artery you are looking at, so the gate is placed on the arterial side (rather than the ventricular). However, sometimes, like in R2A, the turbulent flow might start just before the valve in the outflow tract. Then you would place your cursor in that area. It won’t matter with CW as you are measuring the whole way down the cursor, but it will matter with PW (although usually the flow is too fast for PW).
I know that for TV or MV PW we place the gate at the tip of the valve leaflets, does this apply for the PV and AV?
This is only for E and A waves, so this will only apply to inflows, otherwise for regurgitation you place the cursor as above 🙂
Hi Julia,
Mesothelioma is so tricky!! It is REALLY hard to diagnose and can even be missed on histopathology, although there has been some work around immunohistochemistry use, but this is still pretty limited. Therefore, even if you have histopathology of the pericardium/ pleura it won’t always show mesothelioma. It is something I warn owners about. It is also very difficult to treat, you can perform intra-cavitatory chemotherapy (this is what they do in people), but my experience of that is limited I’m afraid (mainly because by the time dogs are diagnosed most owners will choose euthanasia). Survival is varied – some dogs will have aggressive disease and others will have a more protracted course, the use of pleural ports can be useful in some cases. Unfortunately, by the time it is diagnosed it is usually affecting the pleura and pericardium. If it is just pericardial, we can’t remove the whole pericardium due to its association with the base of the heart so it is a nasty neoplasm to have!
Hope that is useful.
LizReplying to Ornella R. 08/02/2026 - 19:05
Hi Ornella,
I would need to look at her file again to be sure, but I don’t think we found a cause and, given the prognosis, the owners didn’t want to investigate very much. We did the standard UPC and this was WNL, no evidence for Cushing’s either.
Sorry I can’t answer that one!
Liz
Replying to Ornella R. 08/02/2026 - 19:18
HI Ornella,
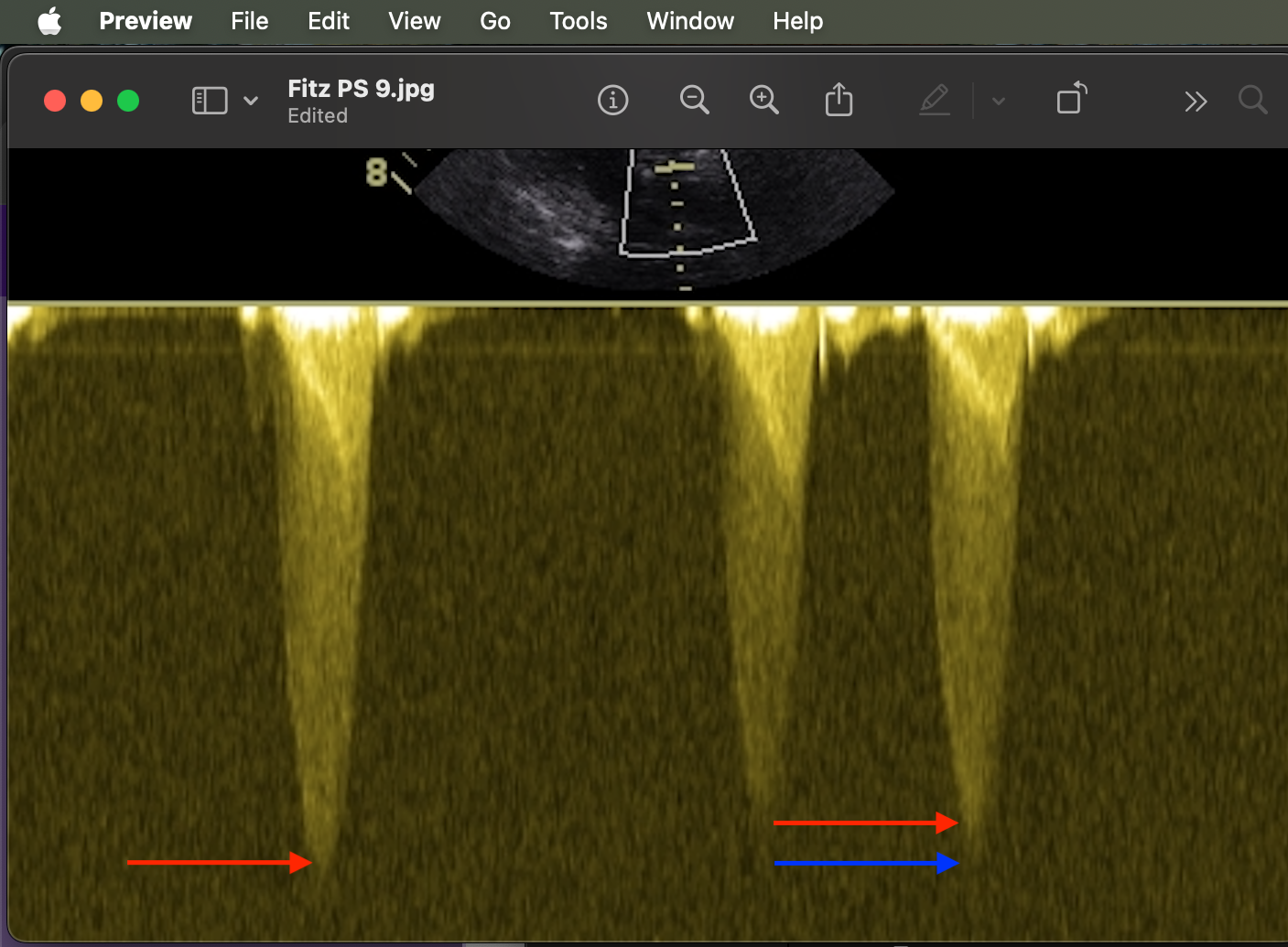
Thanks for the question. Generally you will get a dense appearing profile (termed the ‘chin’) and a fainter area of spectral broadening (termed the ‘beard’). We measure the velocity to the chin and ignore any of the fluffy-stuff that will make the velocity faster than it is. In the attached image the red arrows are the chin and blue the beard.
Hope that is helpful.
Liz
-
AuthorPosts