Liz Bode
Forum Replies Created
-
AuthorPosts
-
Replying to Ornella R. 15/02/2026 - 21:51
Hi Ornella,
When measuring turbulent jet velocity: we identify the jet with colour doppler and in order to get an accurate velocity, we place the CW gate in the neck of the jet (vena contracta), is this correct?
Yes, that is correct, or just on the atrial side of the valve within the colour variance if there is TR or MR.
When measuring PA and AO velocities with CW or PW: do we place the cursor gate across the valve, just below or just above?
This depends on where you see the colour variance start. For the most part the turbulent flow will be within the major artery you are looking at, so the gate is placed on the arterial side (rather than the ventricular). However, sometimes, like in R2A, the turbulent flow might start just before the valve in the outflow tract. Then you would place your cursor in that area. It won’t matter with CW as you are measuring the whole way down the cursor, but it will matter with PW (although usually the flow is too fast for PW).
I know that for TV or MV PW we place the gate at the tip of the valve leaflets, does this apply for the PV and AV?
This is only for E and A waves, so this will only apply to inflows, otherwise for regurgitation you place the cursor as above 🙂
Hi Julia,
Mesothelioma is so tricky!! It is REALLY hard to diagnose and can even be missed on histopathology, although there has been some work around immunohistochemistry use, but this is still pretty limited. Therefore, even if you have histopathology of the pericardium/ pleura it won’t always show mesothelioma. It is something I warn owners about. It is also very difficult to treat, you can perform intra-cavitatory chemotherapy (this is what they do in people), but my experience of that is limited I’m afraid (mainly because by the time dogs are diagnosed most owners will choose euthanasia). Survival is varied – some dogs will have aggressive disease and others will have a more protracted course, the use of pleural ports can be useful in some cases. Unfortunately, by the time it is diagnosed it is usually affecting the pleura and pericardium. If it is just pericardial, we can’t remove the whole pericardium due to its association with the base of the heart so it is a nasty neoplasm to have!
Hope that is useful.
LizReplying to Ornella R. 08/02/2026 - 19:05
Hi Ornella,
I would need to look at her file again to be sure, but I don’t think we found a cause and, given the prognosis, the owners didn’t want to investigate very much. We did the standard UPC and this was WNL, no evidence for Cushing’s either.
Sorry I can’t answer that one!
Liz
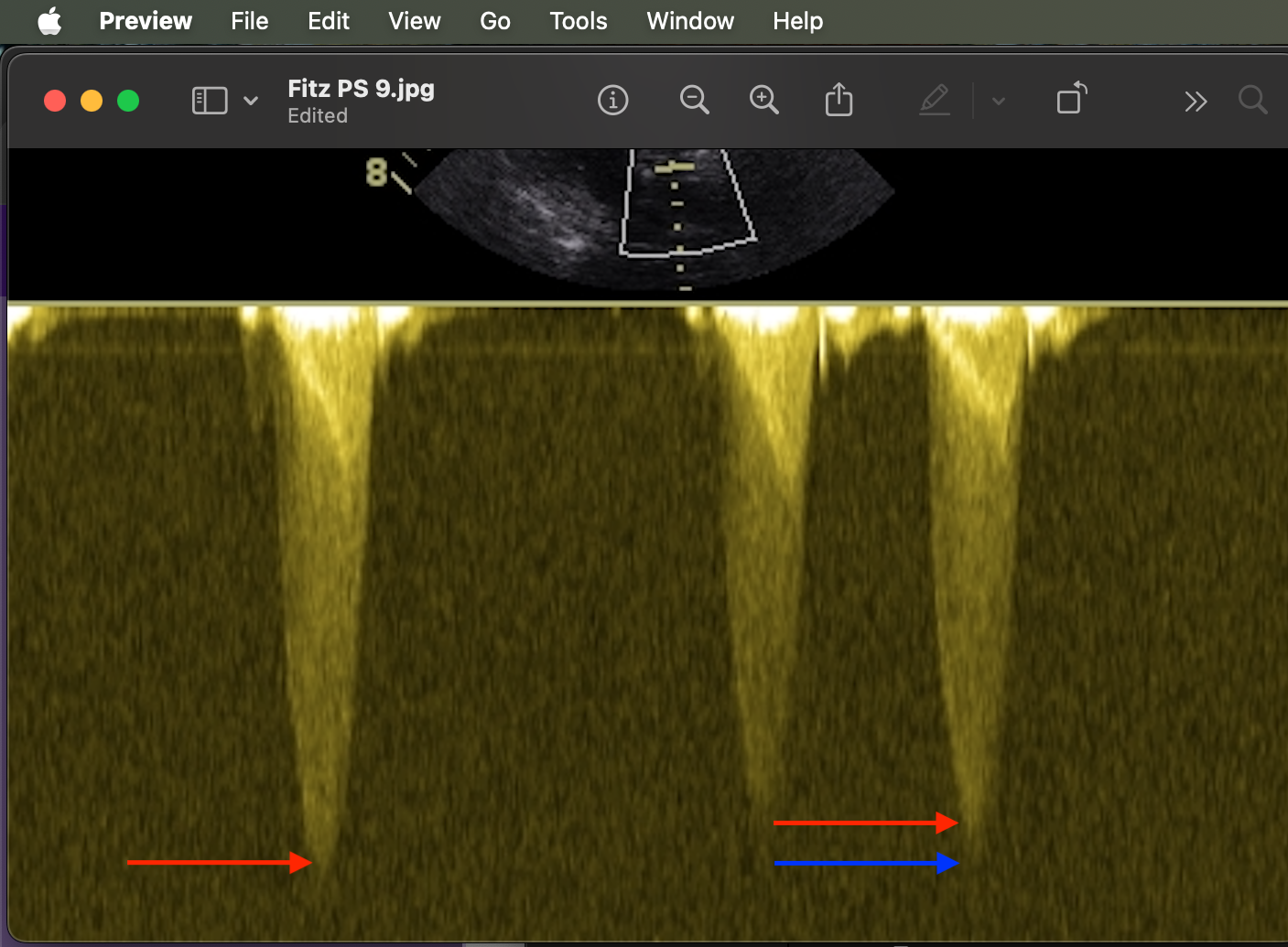
Replying to Ornella R. 08/02/2026 - 19:18
HI Ornella,
Thanks for the question. Generally you will get a dense appearing profile (termed the ‘chin’) and a fainter area of spectral broadening (termed the ‘beard’). We measure the velocity to the chin and ignore any of the fluffy-stuff that will make the velocity faster than it is. In the attached image the red arrows are the chin and blue the beard.
Hope that is helpful.
Liz
Replying to Annet Krabbenborg 19/01/2026 - 21:34
and here you go for these ones:
Which ultrasound do you prefer for cardiac scans?
Do you mean which machine? I use a GE Vivid and I like the GE machines, but the Philips one give really nice 2D images too. If you mean probe than a phased array probe.
And how much time do you think is reasonable to book off for a heart scan, report and make a plan? Of course should get quicker with practise…
Yes, of course it gets quicker and easier with practice.A straightforward MMVD could take me a total of 20 minutes to echo both sides, measure and report! I guess intially an hour per scan/ measure and report would be about right, depending on how many you do in a day that would leave you time to catch up etc.And when is it useful to do pa vti? Is that when checking pulm flow/check re pulm hypertension?
VTI I mainly use that to look at the severity of PS, looking at the ratio of aortic vs pulmonic VTI. I also use it for shunt ratios. I don’t tend to use it for PHT and I don’t use it every day.🙂
Replying to Annet Krabbenborg 18/01/2026 - 15:52
Hi Annet,
Sorry for the delay in replying, I had a really busy week at work so just haven’t had chance to check anything until this evening! I will answer each question in turn below:
– you mentioned torasemide as a rescue diuretic. And you prefer bid dosing? Why is that? I have used it but only use bid dosing if on higher dosages (>0.6mg/kg). How do you swap over from fur to torasemide in stable and unstable patient?
You can use torasemide as a first line diuretic once a day, and I do do that if the animal is tricky to medicate. I use torasemide in my stage D though normally. It has been shown in several studies that it has a t1/2 of about 10 hours so we use it twice daily to try and maintain both plasma levels and renal levels. We take the total daily dose of furosemide e.g. 10/mg/kg/day, and divide that by 1/10th-1/20th dose and then split that into two for BID dosing. We tend to use IV furosemide in an unstable patient before transitioning to torasemide, and I would only swap from furosemide to torasemide orally if the RRR were mildly elevated or we were struggling to control congestion, with the need of escalating the frusemide dose quickly.And you mentioned you can use furosemide cri? How do you do that? Which dose? And just furosemide or i vaguely remember to dilute it with hypertonic saline and dextrose?
We use it after a 2mg/kg IV bolus, then swap to CRI at 0.5-1mg/kg/hr. You tend to dilute it in D5W to keep it iso-osmolar and remember it is light sensitive!
-xrays… i dont do them much anymore since t pocus…? Is that wrong? And did you say you could have no b lines but still be in chf? I usually use microconex abd probe but can you use a phased array heart probe too?
Not wrong no, I POCUS but is an animal isn’t responding as I think they should then I will radiograph them to make sure I haven’t missed something. Micro-convex probes can be better to pick up B-lines but you can use phased-array too. B-lines should be present usually in CHF, but if you have an animal treated for CHF then there could only be 1 or 2 and that can also be normal!
– in lily’s case you mentioned most likely she’s got PH ? I assume this doesnt need treatment with sildenafil unless causing syncopes?
We don’t treat PH in stage C/D dogs usually before we try and control their congestion. You can overload the LA in theory and worsen CHF. However, if we optimise treatment and the PH remains then we might include sildenafil if they are symptomatic or if the Tr velocity is high on echo. They don’t have to be syncopal for us to use it.
– is telmisartan safe in heartdisease? Mvd st b2? And what about if in chf? I wondered if you could use that to treat the hypertension in stead of amlodipine? I assume amlodipine safer as already on benazepril?
You could use telmisartan. I am not aware of any papers that looks at their use in CHF in dogs. We don’t use ACEi in stage B2 so I don’t see why we would use telmisartan in these cases either. You could use it to treat the hypertension, but amlodipine is ‘better’ at reducing systemic hypertension usually so that would be our first line. Amlodipine also reduces afterload to a greater extent, so if a stage C dog was on an ACEi already and then developed hypertension amlodipine would be chosen and would hopefully reduce afterload enough to even reduce MR and LAP!
Hope that all makes sense.
Liz
Replying to Annet Krabbenborg 16/01/2026 - 16:24
Hi Annet,
It is common to have more than 1 congenital abnormality, but CTD is pretty rare. I have only seen a handful of cases. They usually respond well to balloon and RCHF resolves, they generally carry a good prognosis. PS will probably be the one causing the issue (if CTD was treated successfully) and if the dog is in RCHF at one years of age the prognosis is not great. We have no data on prognosis, but I’d say anecdotally that the dog will be unlikely to reach 2 yrs old. If there are no financial limitations then a second procedure could be considered, but this depends on what is causing the RCHF – is it the PS, the CTD or a combination of both?
Liz
Hi Svetlana,
I don’t really like looking for a PDA from the right parasternal view as it is very difficult to distinguish it from the LPA as you say. If we do see one it is mainly through having continuous flow on colour Doppler and then being able to demonstrate a continuous flow on spectral Doppler. That being said, it is always at an angle for me so I prefer to move to the left cranial view!
Pulmonary insufficiency should look like a jet of red originating from the pulmonic valve, not from near the branch of the PA, so should be very different. You would also hear a characteristic continuous murmur. If there is bidirectional or R-L flow then you have more of a difficult time seeing a PDa on 2D and colour – you would need to find evidence for pulmonary hypertension and then a rule out, using contrast study, would be a R-L shunt in a young animal.
If you have a PDA and PS then this can be tricky, you should still have a continuous murmur. When you interrogate the PA you should still see flow that occurs in diastole and systole – this is where moving frame by frame with an ECG is really important.
Hope that helps!
Liz
Replying to Janet Lewis 07/01/2026 - 20:43
Hi Janet,
How interesting! I think it is most likely to be a neoplasm if it is mainly associated with the wall and in a dog with that history – myxomas tend to occur in the LA/LV but not beyond possibility that it could be that. I have also seen RA chemodectomas and other weird and wonderful things. A would think a clot and endocarditis are less likely but you do right I think to provide multi-modal therapy. Also worth evaluating urine UPC? If we think it could be a clot.
Let me know how you get on with it!
Liz
Replying to Annet Krabbenborg 09/01/2026 - 14:57
Hi Annet,
Sadly not. June Boon’s book on echocardiography has tables of some of them in, otherwise you end up searching for them separately. I then print them out and have them in a folder in my room. The breeds we most commonly see are:
English springer spaniels
Whippets/ other sight hounds
Doberman
Boxer
Lab
Great DaneMost of the giant breeds have papers. Sorry that isn’t much help for you.
Liz
Replying to Janet Lewis 06/01/2026 - 15:39
Hi Janet,
this could be a number of things. I have never seen endocarditis of the pulmonic valve in a dog/ cat, but that doesn’t mean it can’t happen!
A few questions:
– what is the signalment?
– what is the clinical history, is it compatible with endocarditis?
– Is the mass attached to the leaflets and mobile?This could be a neoplastic lesion/ thrombus (sterile)/ infectious from that image – it looks pretty big and I guess clopidogrel wouldn’t go amiss just in case!!
Looking forward to your reply, it is an interesting one!
Liz
Replying to Roland R. 05/01/2026 - 11:01
Hi Roland,
I don’t have one I am afraid, but let’s see if Sid does. He finished his residency at Liverpool not so many years ago and I am pretty sure they had a sheet there with some reference ranges on etc. We will get back to you 🙂
Liz
Hi Scott,
Some cardiologists are using this product, and I have seen one or two UK cardiologists talk about it on forums. The experience over here will be limited due to the financial implications, I have not used it. However, it has some very positive data in people and I think it could be beneficial in dogs. Would be interested to hear how your case goes!
Liz
Replying to Annet Krabbenborg 27/12/2025 - 15:01
Hi Annet,
I will do my best to answer the questions so that you can visualise what I mean:
– measuring ivs i know you said leading edge to trailing edge.. ? Do you measure the full ivs (? I assume there’s a left and right side?) or if you can see the divide just the left side of the ivs? Maybe this is not a thing but am sure i’ve heard something re this before)
Yes, there is often a difference in echo texture between the right and left side of the septumn However, there is no consensus on where to measure and as we don’t see this divide on all patients we measure the whole of the septum, leading edge to trailing edge on 2D.– mapse& tapse ? What are normal measurements for cats?
Here is Illaria’s paper on MAPSE and TAPSE in cats (open access) it has all the measurements in there including ref ranges.
https://onlinelibrary.wiley.com/doi/10.1111/jvim.14697– i often struggle to get a really nice la/ao view in a cat ( i often get it more like on a dog echo so la more on left side of the screen in stead of underneath the ao) ? Any tips to improve this?
I think cats atria often do look the same as dogs? Perhaps as they get bigger then they become more ‘underneath’ the aorta. As long as you are seeing a symmetrical looking aorta with the 3 cusps and the body and auricle of the LA in entirety then I think you are doing a good job 🙂
– how do you get the left crannview for the measurement of the lau velocity?
This is tricky in cats with normal left atria, it is much easier when the atria is dilated. You start at the left cranial view with the aorta running horizontally across the screen and then angle your probe slightly caudally so it’s pointing towards the spine near where the last rib inserts. This should bring the auricle to the top oof the screen. In cats with normal LA you will struggle to get it. In those cases I don’t measure it, just LA fractional shortening.Happy New Year 🙂
Liz
Replying to Caroline T. 24/12/2025 - 16:27
Hi Caroline,
This is a good question, what we mean by ‘normal’ velocity is the velocity we would expect to be generated by the right or left ventricle. Trivial MR or TR, in isolation (without valve changes) could be normal but if you are able to interrogate MR and TR and get a good profile then you probably have more than trivial regurgitation and that isn’t ‘normal’.
The RV is a low pressure system normally, so you would anticipate velocity of TR to reflect that, so a normal value for this is <3.0m/s. It is elevated in Pulmonic stenosis and pulmonary hypertension, amongst other more weird congenital abnormalities.
The LV is a high pressure system, so at normal blood pressure you would expect to see an MR velocity of 5-6m/s, reflecting a blood pressure of 100-120mmHg. MR velocity will be higher than this if there is aortic stenosis or systemic hypertension. It will be lower than this if there is increased left atrial pressure/ poor systolic function. However, in order to interpret the velocity of any jet accurately you must be critical of the profiles on Doppler you get, if you don't get a full profile then you can't interpret the image accordingly.
Hope that makes sense.
Liz
-
AuthorPosts